
 By Rita Shane, PharmD, FASHP, FCSHP
By Rita Shane, PharmD, FASHP, FCSHP
Chief Pharmacy Officer and Professor, Department of Medicine
Cedars Sinai Medical Center
Assistant Dean of Clinical Pharmacy
University of California San Francisco School of Pharmacy
March 24, 2021
My career focus has always been on how to balance the total cost of care, particularly in the area of drug therapy, with ensuring quality and safety for patients. Comprehensive medication management is the best way to avoid medication problems and stop wasting lives and wasting money.
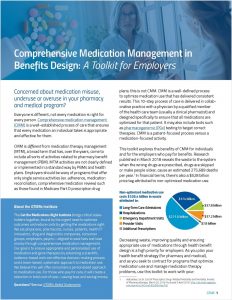
Medication problems generally fall into three “buckets”: overuse of medications that don’t improve health and may cause harm; underuse of critical drugs needed for acute or chronic health problems; and misuse of medications such as opioids. All three can contribute to higher costs and impact patient health.
Overuse is one of the most common issues I see as a clinical pharmacist. In collaboration with the American Society of Health System Pharmacists, I worked with the ABIM Foundation to develop the medication recommendations for the Choosing Wisely campaign, an evidence-based roadmap to help doctors and patients talk about treatments and ask questions so we can reduce preventable harm from medication overuse. It includes detailed guidance for physicians on hundreds of tests and medications that, used out of context of the patient’s entire medication picture, won’t help and may cause harm.2 The bottom line: To prevent overuse of medications, health care providers shouldn’t start or continue medications without a comprehensive evaluation of the patient’s health issues and medications.
That’s why CMM should be part of the care process for the kind of patient I tend to see, the high-risk patient. They typically fall into one of three categories:
- Poly Problems: Patients with multiple health issues being treated by multiple medications prescribed by multiple treating physicians;
- Patients transitioning from one level of care to another: For example, when a patient is discharged from an acute care stay at a hospital to long-term care, to a rehabilitation facility, or back home, errors can occur when they begin taking medications they were prescribed before the hospital stay that are no longer appropriate, or if they stop taking medications because discharge orders were unclear; and
- Cancer Patients: These patients typically are prescribed multiple medications and are struggling to balance medical care costs with changes in their work and life because of the disease. These socio-economic issues affect whether patients fill prescriptions on time and are able to take them as prescribed.
The common factor with high-risk patients across all three categories is the lack of any single provider managing the whole patient picture. That is where the clinical pharmacist can add incredible value by taking on the role of medication expert on the health care team and systematically evaluating all the patient’s health issues, medications, lifestyle factors and desired health goals to optimize medication regimens.
CMM puts the brakes on medication overuse problems like a prescription cascade, which happens when a patient is on one drug to treat a condition, and then is prescribed another drug either for a new condition or to counter a medication side effect. For example, a patient with diabetes is newly diagnosed with high blood pressure and prescribed Amlodipine by her cardiologist to treat it, and then notices her feet and hands are swelling (a condition that happens in 9% of patients on this drug). Her primary care physician prescribes a diuretic to reduce the swelling, which causes urinary incontinence. A urologist prescribes a third drug to treat the incontinence, which causes dry mouth, so her primary care physician writes a fourth prescription to treat that condition. None of these physicians is evaluating whether the initial high blood pressure medication was the right choice for this patient, nor how this medication cascade is affecting the patient’s insulin levels.3
Hospitals, emergency rooms and physician practices are already required to assess all medications and keep an accurate record so that information is known and evaluated when new issues arise. But these lists are notoriously inaccurate; a 2019 study found that up to 80% of older patients have at least one medication error when they’re discharged from the hospital.4 If these errors aren’t caught when a patient is admitted, or if medication lists aren’t updated to reflect treatments that began or were discontinued during a hospital stay, it’s entirely possible that a patient who was admitted because of an adverse drug event or medication error will be discharged with instructions to restart regular medications—including the ones that caused the hospitalization to begin with. It’s a vicious cycle. Think about the patient discharged to a skilled nursing or rehabilitation facility after a hospital stay, who may not be equipped themselves to accurately assess the medications on their discharge documents.
Specialty pharmacy medications are already under scrutiny because many have very high costs. Most have specific criteria around who should take them and contraindications for their use. Although very effective when used correctly, they can also cause harm if they’re not optimized in the context of a patient’s whole health. They should be evaluated with full knowledge of other medications being used and other health conditions. When the specialty pharmacy benefit is carved out, it can actually increase costs because these medications are being managed in a silo.
So, start saving lives and saving money. Your workforce is a population that is best served when it has the resources to achieve optimal health. CMM is a critical part of a team-based population health approach that identifies medication problems and mitigates risk.
Click here to sign up for an advanced copy of the Employer Toolkit coming in April
The GTMRx Institute recognizes that employers as health plan sponsors manage the health benefits for 49% of this country’s total population. We also know because they sign the check, they have much to gain from optimizing the medications involved in 80% of all medical treatments.
This toolkit explores the benefits of CMM for individuals and for the employers who pay for benefits. Research published in March 2018 reveals the waste to the system when the wrong drugs are prescribed, drugs are skipped or drugs make people sicker which in turn leads to an estimated 275,689 deaths per year. In financial terms, there’s also a $528 billion price tag attributed to non-optimized medication use.
Use this toolkit to work with your:
- Pharmacy Benefit Managers (PBMs)
- Medical carriers
- Benefit consultants
- Solution providers (PGx, others)
- Employees
This toolkit was developed with guidance and support from the GTMRx Employer Toolkit Taskforce.
- Excerpted from the July 23, 2020 presentation to the GTMRx Employer Task Force
- Ds. (2020, April 22). Choosing Wisely. Retrieved January 09, 2021, from https://www.choosingwisely.org/
- Nguyen, P. V., & Spinelli, C. (2016). Prescribing cascade in an elderly woman. Canadian pharmacists journal : CPJ = Revue des pharmaciens du Canada : RPC, 149(3), 122–124. https://doi.org/10.1177/1715163516640811
- Graabæk T, Terkildsen BG, Lauritsen KE, Almarsdóttir AB. Frequency of undocumented medication discrepancies in discharge letters after hospitalization of older patients: a clinical record review study. Ther Adv Drug Saf. 2019;10:2042098619858049. Published 2019 Jun 16. doi:10.1177/2042098619858049
Related



